Health care utilization for chronic musculoskeletal pain risk: Lessons from the CRASH study
Each year, over four million people go to U.S. Emergency Departments (ED) after a motor vehicle crash (MVC). Although the vast majority of patients are sent home without any serious injuries, many will experience aches and pains such as whiplash and back strains. While many patients get better in the first couple of weeks after an accident, almost half of the people who have gone to the ED after an MVC will continue to have pain several weeks later. The treatment that is started in the ED may impact pain in the weeks to even months after the initial ED visit. Current treatments include physical therapy, pain medications, and behavioral therapy, alone or in combination. After leaving the ED, patients may also receive treatment from their primary care doctor, specialists, or other providers. Currently, it is not known how people use each of these health services as part of recovery from an MVC and what the best course of treatment is.
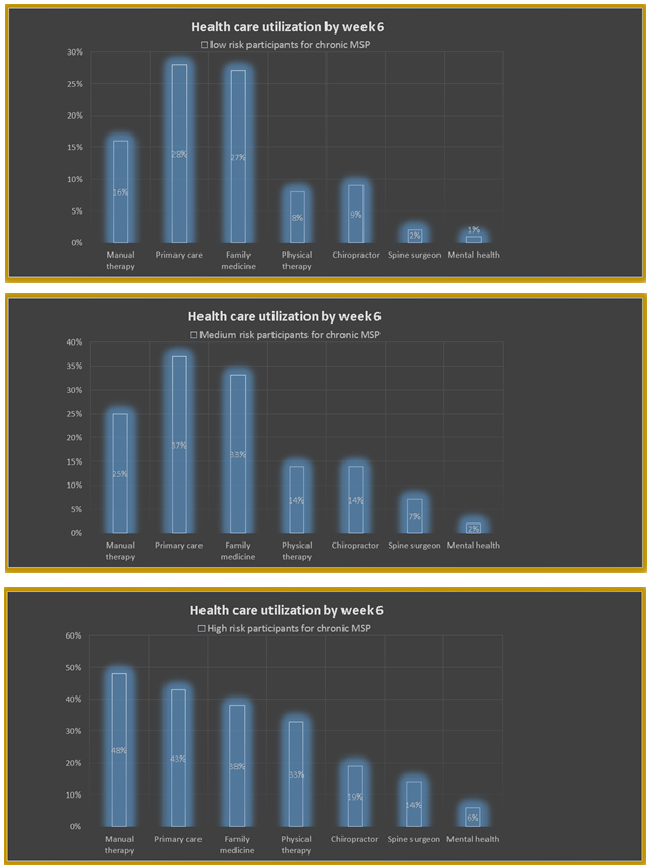
Fig. 1. Health care utilization by week 6 across low, medium, and high-risk participants.
A study was conducted to understand which health services patients most often use following a MVC. This study included participants from eight hospitals across four states. A total of 793 participants were followed up for one year and were asked to complete a survey on the different types of health services they may have used after their MVC. Participants were divided into high, medium and low risk groups depending on the possibility of them developing long-term pain following their MVC.
The study findings revealed that participants in the high risk group had a greater chance of developing long-term pain in comparison to those in the medium or low risk groups. It also revealed that across the three groups, some of the most commonly used health services included visits to Primary care, Family medicine, and Physical therapy providers. In comparison, usage of Mental health services was extremely low.
Additionally, the study findings showed that less than half of the participants in the high risk group received appropriate health services. These findings express the need for more organized access to health services for the prevention and treatment of pain in MVC patients. Providing patients with education and referrals to suitable resources may also prevent the over-use of certain health services and avoid unnecessary medication use if pain is controlled in another way. Early access to mental health services may also prevent and improve pain after trauma, but mental health services were rarely used.
There is opportunity in the ED to make timely health services referrals for patients who are discharged home following a MVC, but might be at high risk of negative health outcomes. Future research should be conducted to evaluate if separating people into different risk groups and providing them with differing types of care is both clinically and cost effective. For example, physical rehab, behavioral therapy, and specialty specific services may have better outcomes for patients who have a higher chance of developing long-term pain. In contrast, providing over-the-counter pain-medication and education on the natural course of pain to those with a lower likelihood of developing long-term pain may avoid unnecessary care.
Taha Feroze, Tarek Nizami, Evelyn K Nimaja, Francesca L. Beaudoin
Department of Emergency Medicine, Alpert Medical School of Brown University, Providence, RI, USA
Publication
Health care utilization following motor vehicle collision is poorly stratified by chronic pain risk: Lessons from the CRASH study.
Beaudoin FL, Rosellini AJ, Bortsov A, McLean SA
Am J Emerg Med. 2019 Mar

Related Articles:
 | Sleep abnormalities in different clinical stages of… Sleep abnormalities are commonly observed in individuals with schizophrenia and related psychotic disorders. Research shows that over half of people with these conditions have trouble sleeping. Poor sleep also often… |
 | UCLA researchers develop high-sensitivity… A significant advancement for point-of-care medical diagnostics, a team of researchers from UCLA has introduced a deep learning-enhanced, paper-based vertical flow assay (VFA) capable of detecting cardiac troponin I (cTnI)… |
 | The Manikin Challenge: manikin-based simulation in… Psychiatry is a nuanced specialty that relies on body language and subtle nonverbal cues from patients. As such, when using simulation to teach medical students, standardized patients are considered the… |
 | Systemic therapy in juvenile localized scleroderma Juvenile localized scleroderma, also known as morphea, is an rare condition, it occurs around 1 in 5000 children, where the skin and the tissues underneath the skin like fat tissue,… |
 | Looking inside the heart: how multiple chronic… The aim of this study was to understand how having several ongoing health problems—what we refer to as multimorbidity—impacts the heart in people with cardiovascular disease, especially those undergoing heart… |
 | Late second trimester miscarriages A second trimester miscarriage is the spontaneous loss of a pregnancy between 12 and 22 weeks of pregnancy. This is indeed a very sad experience to the parents. It has… |





Leave a Reply
You must be logged in to post a comment.