Nailfold microangiopathy in dermatomyositis and systemic sclerosis: what is different in long term follow-up?
Dermatomyositis (DM) is a chronic inflammatory disorder involving mainly the skin and muscles. Systemic Sclerosis (SSc) is an autoimmune rheumatic disease of unknown etiology characterized by vascular alterations and progressive tissue fibrosis of multiple organs.
Peripheral microangiopathy is typical of SSc, as well as frequently observed in DM, and it can be easily recognized by nailfold videocapillaroscopy (NVC), a non invasive and safe technique. The characteristic NVC pattern named “scleroderma-pattern” that has been typically described in SSc, has also been reported in other “scleroderma spectrum disorders”, including DM. Only few studies described the main NVC changes over time in this last clinical condition.
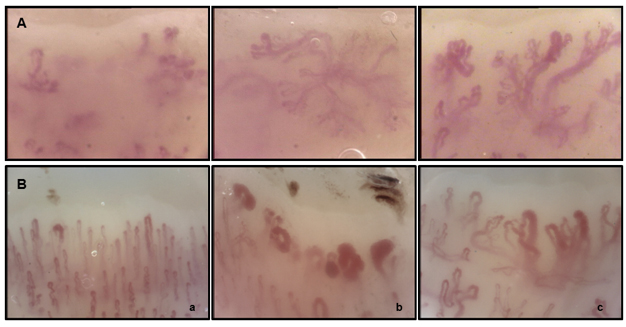
Fig. 1. A: Nailfold videocapillaroscopic pictures during the 3 year follow-up in a dermatomyositis patient (scleroderma-like pattern). B: Example of progression of nailfold videocapillaroscopic patterns during follow-up in a systemic sclerosis patient (a = Early, b = Active, c = Late pattern). Magnification 200x.
The aim of our retrospective study was to describe the main NVC changes in patients with DM,during a three year follow-up, and to investigate possible differences in NVC findings at first visit (first capillaroscopy) in comparison with patients affected by SSc matched for sex, age and disease duration.
Twenty-four DM (mean age 54±15SD years; disease duration 4±5 years; 4 males and 20 females) and twenty-four SSc patients (mean age 55±13 years; disease duration 4±5 years; 4 males and 20 females) matched for age and disease duration at first NVC have been retrospectively evaluated. The following qualitative parameters have been assessed by NVC: enlarged loops (irregular or homogeneous increase of capillary diameter ≥20 but <50 μm), giant capillaries (homogeneously dilated loops with a diameter ≥50 μm), microhaemorrhages (dark masses attributable to hemosiderin deposit), ramified capillaries (abnormally shaped capillaries, branching, bushy, interconnected, originating from a single capillary, expression of angiogenesis), disorganization of the vascular array, capillary density (number of capillaries per linear millimetre on first row). The microangiopathy evolution score (MES) was also calculated.
In this study nineteen out of 24 DM patients (79%) showed a NVC “scleroderma-like pattern” at baseline.
Comparing at baseline DM with SSc patients, the giant capillary and microhaemorrhage scores were significantly higher in SSc than in DM patients (p=0.04, and p=0.05 respectively), while capillary density, ramification and disorganization scores were higher in DM than in SSc patients (p=0.05; p=0.002; p=0.004, respectively). The absolute number of ramified capillaries was significantly higher in DM patients (p=0.002), while the absolute capillary number was significantly higher in SSc patients (p=0.05) at baseline (Tab. 1).
No statistically significant variations of all the capillaroscopic scores was observed during the 3 year follow-up in DM patients (Fig. 1A), differently from SSc which microangiopathy is notoriously progressive (from the “Early” to the “Active” and finally to the “Late” pattern) (Fig. 1B).
By comparing DM patients with or without anti-Jo-1 antibody positivity, no statistically significant differences of the scores of the main capillary parameters was observed at baseline between the two groups. In our study, a relevant angiogenesis is a distinctive NVC feature in patients with DM: the comparison between DM and SSc patients at baseline demonstrated a particularly higher prevalence of giant capillaries and microhaemorrhages in the latter disease, as well as higher frequency of ramified capillaries (angiogenesis) and loss of capillaries in the former.

Tab. 1. Comparison of nailfold videocapillaroscopic (NVC) parameters at baseline in whole dermatomyositis (DM) and systemic sclerosis (SSc) patients. Means ± standard deviations are reported.
In conclusion, both SSc and DM may display similar nailfold microvascular abnormalities that can be detected by NVC. However, DM an SSc display quite different nailfold capillary features: this open the door toward a possible identification of a DM capillaroscopic pattern (different from the well known scleroderma pattern of SSc), which may be of great relevance for the early diagnosis of connective tissue diseases.
M Cutolo, A Sulli, C Pizzorni
Research Laboratories and Academic Division of Rheumatology Postgraduate School of Rheumatology,
Department of Internal Medicine – University of Genova – IRCCS San Martino Polyclinic Hospital, Geneva, Italy
Publication
Long-term follow-up of nailfold videocapillaroscopic changes in dermatomyositis versus systemic sclerosis patients.
Pizzorni C, Cutolo M, Sulli A, Ruaro B, Trombetta AC, Ferrari G, Pesce G, Smith V, Paolino S
Clin Rheumatol. 2018 Oct

Related Articles:
 | Systemic therapy in juvenile localized scleroderma Juvenile localized scleroderma, also known as morphea, is an rare condition, it occurs around 1 in 5000 children, where the skin and the tissues underneath the skin like fat tissue,… |
 | Exploring gap junction networks required for… The study of pattern formation has advanced to a new phase involving channel molecules acting on bioelectric signals, with gap junctions being major relevant factors. Gap junctions are composed of… |
 | Is multiple sclerosis triggered by immunological… Multiple sclerosis (MS) is an autoimmune disease where immune cells (T cells) and antibodies progressively damage the myelin sheath surrounding nerve cells leading to their loss of function. We have… |
 | Can we accurately diagnose different clinical… Progressive Supranuclear Palsy (PSP) is the second most common degenerative parkinsonian syndrome after idiopathic Parkinson’s disease. PSP is a clinically heterogeneous disorder with several clinical variants. The two most common… |
| Social rank recognition is altered in autism… Humans and many other animals spend their lives in social groups, along with constructing social hierarchy within the groups. Since social hierarchy is a principal determinant for allocation of limited… | |
 | Rabbits with mammary carcinomas as a model for… Within a breeding colony of rabbits, the American pathologist Harry Greene (1904-1969) observed that mammary carcinomas were restricted to certain families. This is suggestive of a familiar predisposition as it… |





Leave a Reply
You must be logged in to post a comment.